
The Liability-Laundering Machine
A Study in How Pharmaceutical Costs and Risks Get Transferred

Introduction
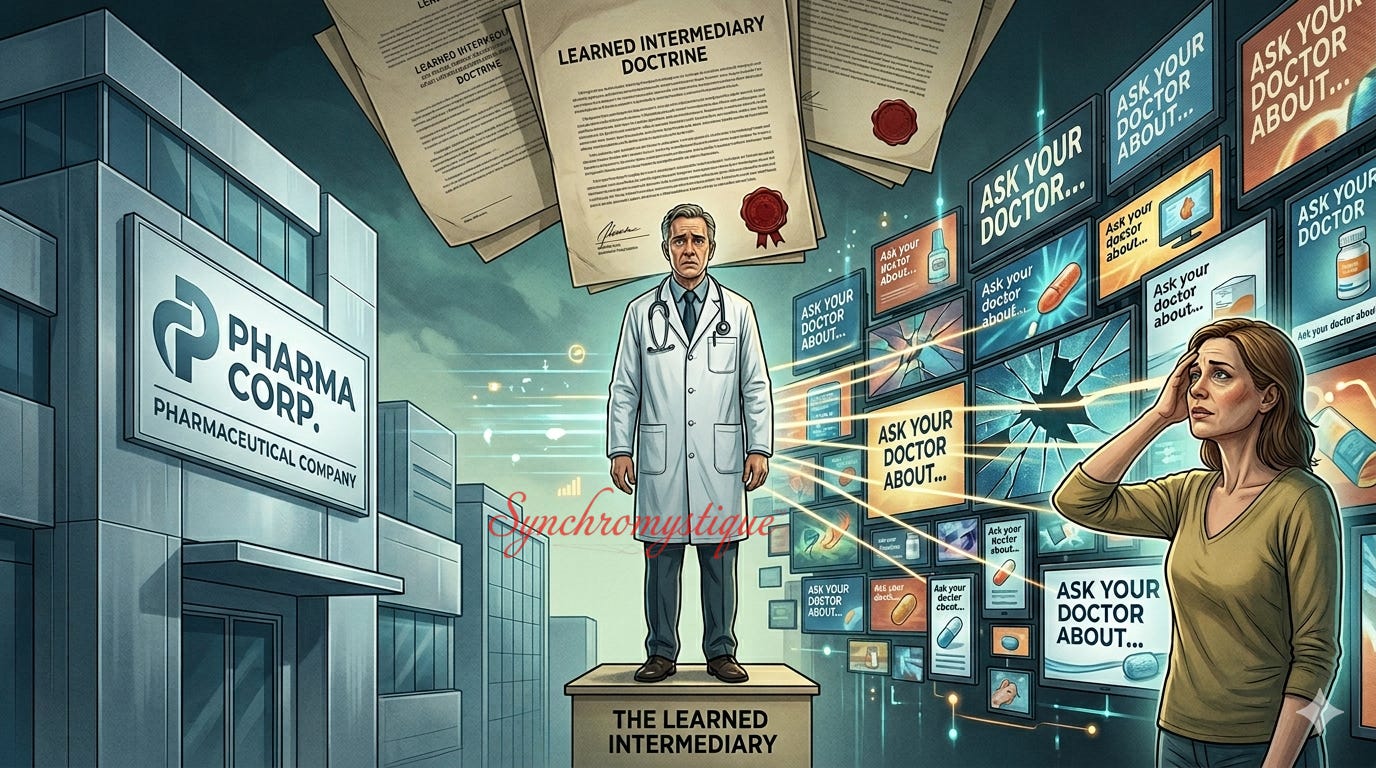
Every pharmaceutical commercial ends the same way. After thirty or sixty seconds of smiling models depicting restored vitality — all carefully curated to kindle audience hope — a voice urges the viewer to “ask your doctor” whether the advertised drug is “right for you.” The phrase is so familiar that it barely registers anymore. Yet it conceals a remarkable legal and institutional contradiction.
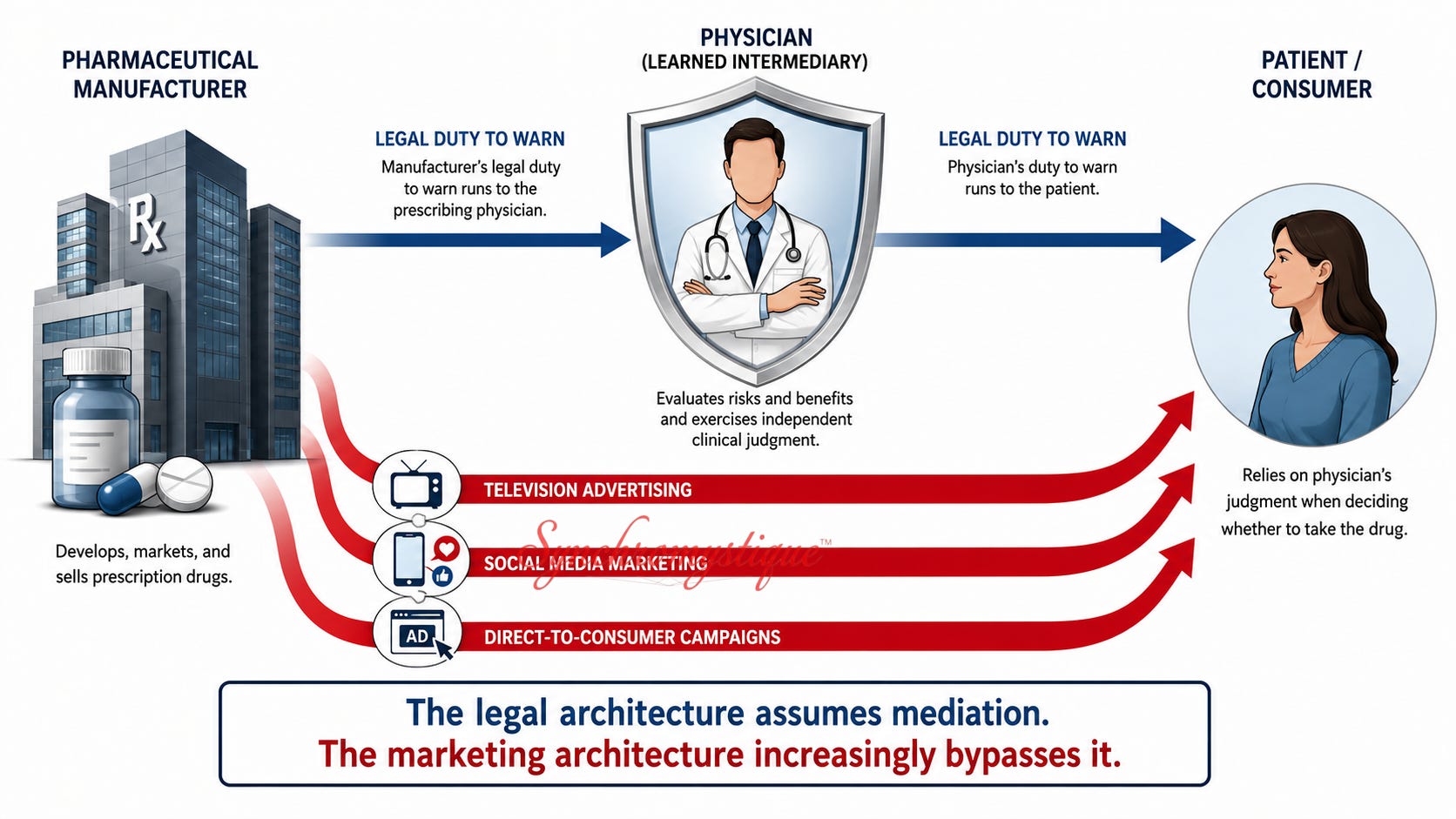
You see, under American law, pharmaceutical manufacturers generally owe their “duty to warn” not to patients directly, but to prescribing physicians. This principle — known as the “learned-intermediary doctrine” — rests on a straightforward assumption: namely, that doctors stand between drug companies and patients, independently evaluating risks and benefits before making treatment decisions. The physician is supposed to function as an intermediary.
And yet…!
The United States is one of only two countries (the other is New Zealand) on earth that permits direct-to-consumer prescription-drug advertising. Let that sink in for just a moment.
The same industry that enjoys legal protection on the grounds that physicians mediate patient decisions spends billions of dollars every year attempting to shape those decisions before any physician enters the conversation. The legal architecture assumes mediation. The marketing architecture increasingly bypasses it. The shield and the spear are wielded by the same hand.
This tension is not an isolated curiosity. Rather, it offers a revealing glimpse into a broader institutional pattern — one that critics of regulatory capture, public-choice theory, and public-private corporatism have been describing for decades.
The modern pharmaceutical industry is often portrayed as a free-market engine of biomedical innovation constrained by imperfect regulation. But there is another way to understand it.
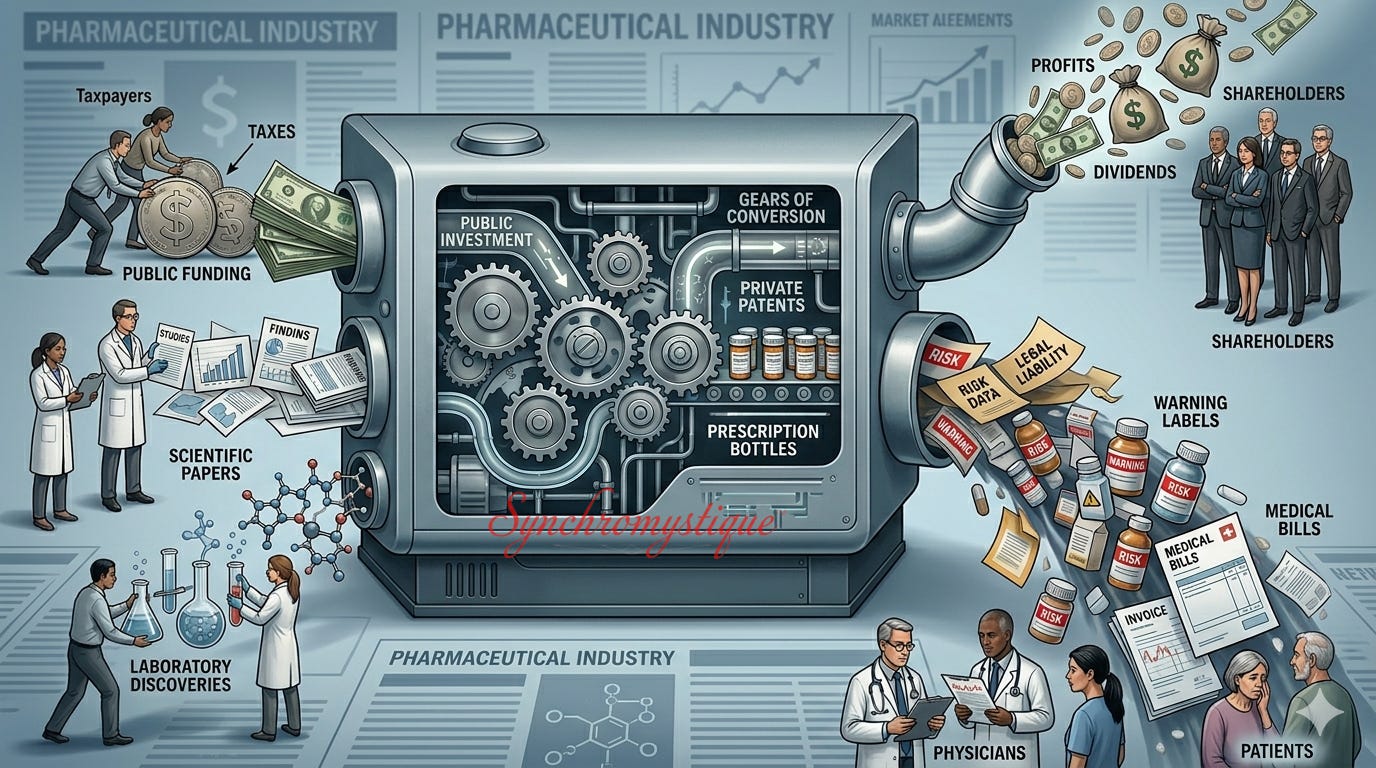
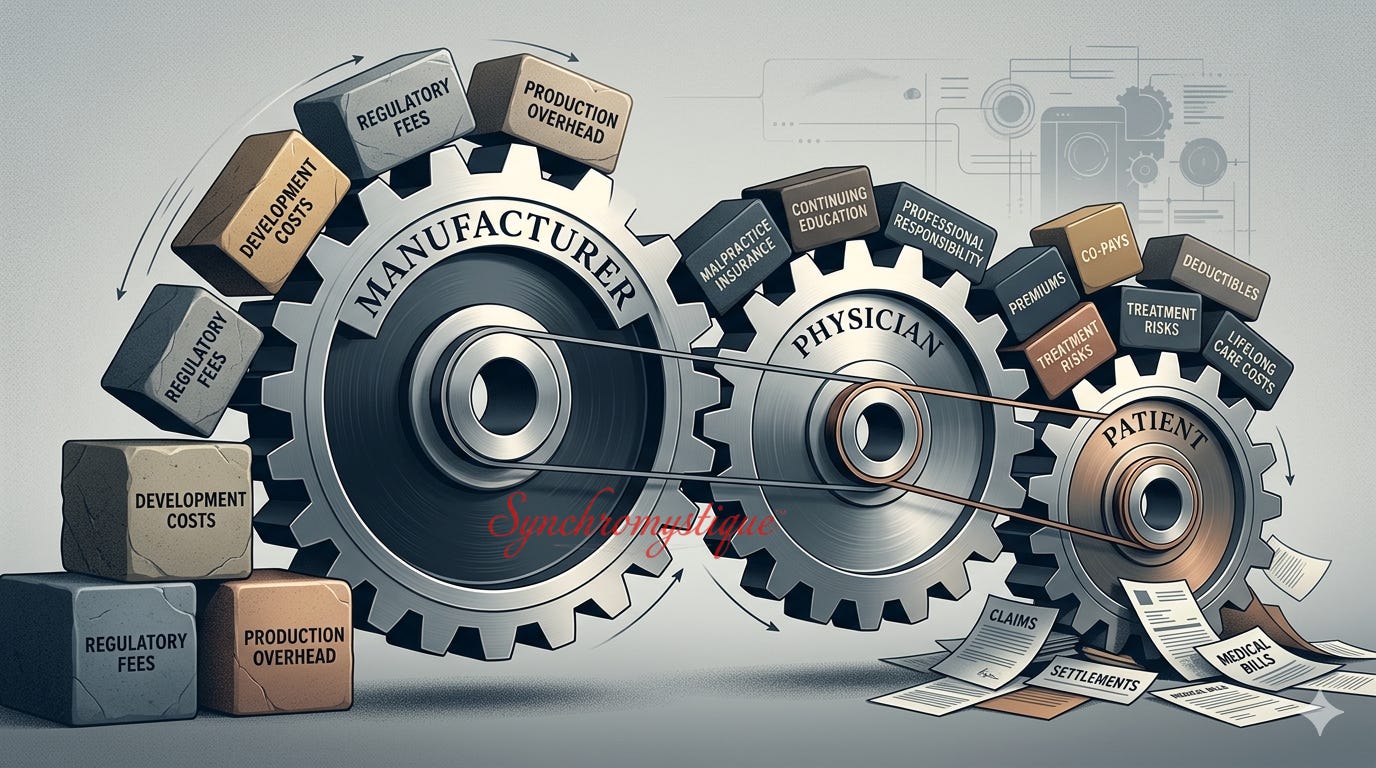
In this alternative interpretation, the industry’s most important achievement is not the mere (and so-called) production of “medicines.” It is the systematic transfer of financial cost, legal liability, testing risk, and moral responsibility away from manufacturers and toward taxpayers, physicians, pharmacists, and — ultimately — patients themselves.
Viewed from this angle, taxpayer-funded research, off-label prescribing, post-market surveillance, package-insert disclosures, repurposing trials, and evolving liability doctrines cease to appear as separate, possibly dysfunctional, phenomena. They become successive stages in a single, purposeful institutional process.
The pattern — part of which is captured by the aphorism socialize-cost / privatize-profit — is both striking and consistent.
The public funds the foundational science.
Private firms acquire exclusive rights to commercialize the resulting discoveries.
Physicians absorb much of the immediate malpractice exposure.
Patients absorb much of the physical risk.
And when the inevitable adverse outcomes emerge, legal responsibility is progressively redistributed downstream through disclosure regimes and liability doctrines that increasingly insulate manufacturers from direct accountability.
The upshot? Profits flow upward. Risk flows downward and outward.
Over time, the industry develops an ever-thicker legal hide between itself and accountability, shedding liability the way living tissue sheds dead skin. What appears as a collection of disconnected doctrines, laws, and policies increasingly resembles a single adaptive process: a literal institutional callusing.
It would be a mistake to characterize this operation as a “conspiracy.” The corporate System functions as described in the open under the academic cover of “Public Choice Theory” and as part of the pervasive “marketization” of all aspects of American life sanctioned by Neoliberalism.
Crucially, what emerged did not depend on secret coordination. On the contrary, it only requires institutional participants to behave predictably and “reasonably” according to the incentives built into the legal and regulatory framework. The actors are said to be instrumentally rational.
The pharmaceutical industry, in this account, has not merely learned how to manufacture drugs. It has learned how to manufacture distance between itself and liability.
The following essay examines the mechanism through which that distance is created and through which “Big Pharma” transforms into a veritable Liability-Laundering Machine.[1]
Caveats and Disclaimers
The following is for general educational, entertainment, or informational purposes only. It is not intended as legal, medical, or any other sort of advice — for which, seek licensed professionals in your area. Nothing here should be understood as overriding the recommendations that you received from trusted physicians, or taken to imply that pharmaceuticals lack therapeutic value or that any specific treatment should be avoided. Instead, what follows is a structural-political analysis in a register of regulatory-capture scholarship and public-interest economics.
The Core Thesis
The modern pharmaceutical system is not merely a subset of the fabled “free market” that happens to suffer from regulatory imperfections (perhaps because, as “right libertarians” might have us believe, government is “too big”). It is actually a publicly subsidized apparatus in which financial cost, testing risk, and legal liability consistently flow toward taxpayers, physicians, and — ultimately — patients, while profits unfailingly flow toward corporate shareholders, investors, and patentees.[2]
This outcome does not require coordination or “conspiracy.” It requires only that each actor behave (instrumentally) “rationally” within a legal and regulatory architecture that has evolved, through decades of targeted legislative and judicial intervention, to produce exactly these incentive alignments.
Stage One: The Nader Loop
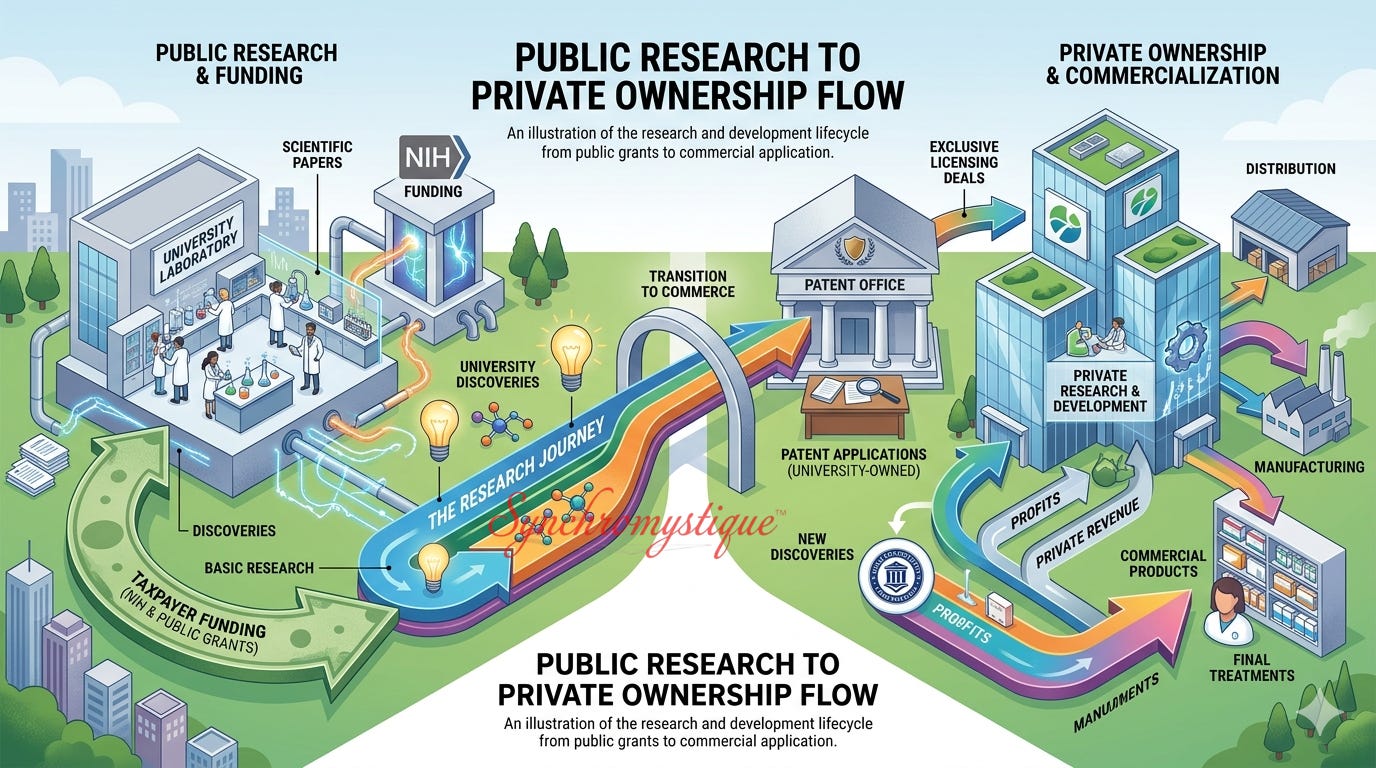
The foundational move is the conversion of public investment into private monopoly. A widely cited 2018 study published in the academic journal Proceedings of the National Academy of Sciences, or PNAS, found that National Institutes of Health, or NIH-funded research contributed to the scientific foundations underlying all 210 drugs approved by the United States Food and Drug Administration (FDA) between 2010 and 2016.
That totaled over $100 billion in public investment.[3]
Basic pharmaceutical research — identifying molecular targets, mapping disease pathways, screening compound libraries[4] — is overwhelmingly conducted in publicly funded laboratories.
The Bayh-Dole Act of 1980 then permitted universities to patent discoveries made with federal funding and license them exclusively to private firms.[5] The effect, as Ralph Nader and his colleagues at Public Citizen[6] have argued, was to leverage “highly questionable evidence”[7] to transform the public research infrastructure into a “corporate-welfare” pipeline that feeds private patent portfolios.[8]
Admittedly, defenders of Bayh-Dole argue that commercialization incentives accelerated the translation of laboratory discoveries into usable therapies. But the rejoinder is that whatever gains were achieved came at the price of privatizing publicly financed research.
The resulting circularity is not subtle. The same taxpayers whose NIH contributions funded the discovery then pay again — at monopoly prices enforced by the patent system — to access it.
The public pays to find the drug. The public pays to buy the drug. The private licensee reaps the financial rewards.
Stage Two: Off-Label Prescribing as Uncompensated Population Trials
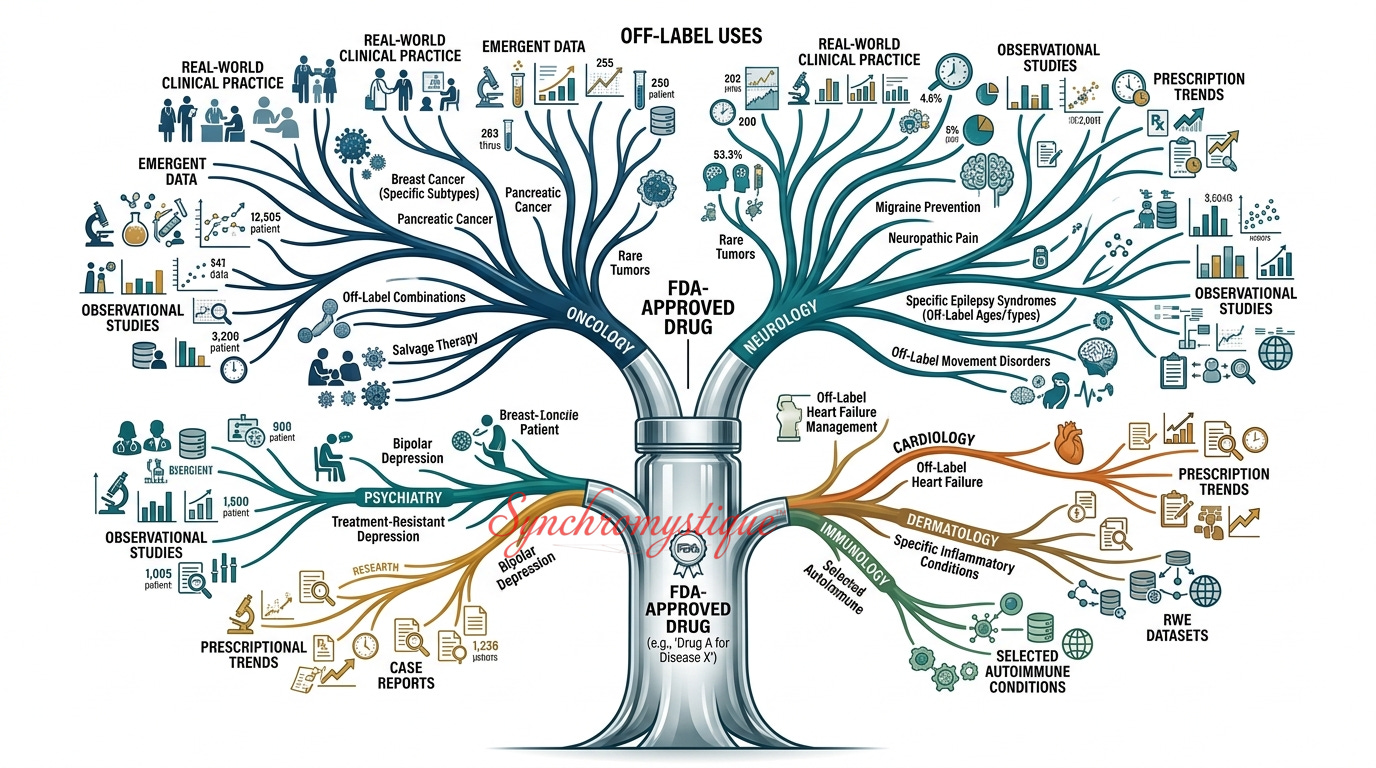
Once a drug receives FDA approval for a primary indication, physicians may legally prescribe it for any condition that they deem clinically appropriate. Admittedly, this is a defensible diagnostic and therapeutic practice with genuine benefits — for example, perhaps in pediatric oncology, because children are routinely excluded from adult pharmaceutical trials and off-label prescription is often the only available standard of care.
But the same mechanism creates a structural incentive for manufacturers to expand market reach without incurring the cost of new clinical trials. Bracketing whatever objections or worries one may have regarding the drug-approval process, it is one thing for a doctor and pharmacist to adjust the dosage of an approved cancer drug to offer hope to a child suffering from the condition the substance was engineered to treat. It is another for, say, chemicals that are approved as antidepressants or antipsychotics to be used instead for eating disorders, headache relief, or as sleep aids.
And it is not exactly a case where physicians “discover” these off-label possibilities on their own, independently of manufacturer influence. Through continuing “medical-education” funding, ghost-written journal articles, conference sponsorships, and — as internal documents in the Neurontin (Gabapentin),[9] Zyprexa (Olanzapine),[10] and Paxil (Paroxetine)[11] cases demonstrated — coordinated sales representative incentive programs, manufacturers have repeatedly encouraged off-label use on a massive scale.
The prescribing physician conveniently (for the pharmaceutical company) absorbs the immediate malpractice exposure. The patient absorbs the ultimate physical risk. Meanwhile, the manufacturer collects revenue and, even more critically, catalogs the adverse event data generated by what functionally resembles a large-scale, uncontrolled source of post-market observational data — if not a massive, uncontrolled, real-world trial conducted without the informed-consent architecture, disclosures, or even the possible compensation that formal clinical trials would require.
The Department of Justice settlements in the relevant cases — $2.3 billion from Pfizer in 2009, $3 billion from GlaxoSmithKline in 2012, $1.4 billion from Eli Lilly in 2009 — should not be taken as evidence that the system “failed.”
Critics have argued that the scale of off-label revenues generated often dwarfed the eventual settlements, creating incentives that made penalties appear manageable rather than prohibitive.
As ex-Wall-Street trader Max Keiser is fond of saying (though addressed to a different economic sector), corporate financial modeling tends to treat anticipated settlement costs as “costs of doing business.” Or, to put it slightly differently again, the penalties functioned as de facto licensing fees — not as meaningful deterrents.
Stage Three: The Data-Harvesting Racket
As adverse events accumulate during widespread off-label use, manufacturers face a structural choice: withdraw the drug from informal market expansion, forfeiting revenue, or incorporate the adverse data into the package insert under subsections with labels like “Adverse Reactions,” “Precautions,” and “Warnings.” The (instrumentally) “rational” choice, consistently, is the latter.
Each label revision does two things simultaneously. Firstly, and admittedly, it improves patient information — a genuine benefit. But the second thing it does is completes a liability transfer.
Under the “learned-intermediary” doctrine,[12] a manufacturer’s legal duty to warn runs to the prescribing physician, not directly to the patient. Once a risk is documented — in black and white, as it were — within the prescribing information, the manufacturer can claim that it has discharged its duty.
Increasingly, there is an irony that is difficult to overstate. The learned intermediary doctrine rests on the premise that manufacturers communicate risk to physicians, who then exercise independent clinical judgment on the patient’s behalf — making direct manufacturer-to-patient communication legally unnecessary. Yet the United States is one of only two countries in the world (the other being New Zealand) that permits pharmaceutical companies to advertise prescription drugs directly to consumers.

Yet, the industry spends several billion dollars annually on direct-to-consumer advertising — television spots, digital campaigns, and print placements that are calibrated to bypass the learned intermediary entirely and cultivate patient demand before any physician has evaluated any claim or data. These advertisements reliably conclude with a variant of the same instruction: “Ask your doctor if [x drug] is right for you.” An influenced patient then arrives at the consultation having already been primed by this marketing. A physician’s “independent” judgment operates downstream of these corporate campaigns. Thus, the doctrine that shields manufacturers from direct liability to patients is paired, in practice, with an advertising-marketing apparatus that targets those same patients directly. The shield and the spear are wielded by the same hand.
Nevertheless, it is then the physician — who prescribes “knowing” (in principle) the disclosed risks — who assumes the duty-to-warn obligation. Finally, the liability transfer is complete when the patient voluntarily has his or her prescription filled and takes the drug. Legally, he or she receives the informed prescription and thereafter takes on, under the doctrine of voluntary assumption of risk, the residual liability for those presumptively disclosed harms.
The package insert, in other words, functions simultaneously as a public health document and as a liability instrument. Documenting an adverse effect transforms it, in legal terms, from an undisclosed design hazard into a disclosed and assumed risk.
A candid observation is warranted here. The learned intermediary doctrine functions as a coherent liability-transfer mechanism only if the intermediary — the prescribing physician — actually reviews and communicates the package insert’s risk disclosures to the patient. In clinical practice, this is largely a legal fiction.
Package inserts are not consultation documents, nor are they particularly patient-friendly. They are dense, multi-page technical instruments that few physicians discuss systematically with patients, and that most patients never read on their own.
The operative assumption in the examination room is simpler and more intuitive. If a physician prescribes a drug, then the benefits are presumed to outweigh the risks in that patient’s case. Trust the doctor.
The deeper problem is not physician negligence. It is that everyone downstream of the manufacturer — physicians, pharmacists, and patients alike — tends to operate on an implicit prior assumption: namely, that a drug would not have reached the market unless it were, in some meaningful sense (and as relentless advertising has declared) “safe and effective.”
Arguably, that is not an evidence-based conclusion. It is, increasingly, an article of faith — and one that has been cultivated, with considerable sophistication and at enormous expense, by the same industry whose liability the learned intermediary doctrine is designed to contain.
The marketing apparatus that produces the faith and the legal architecture that exploits it are, once again, engineered by the same people and operated by the same hands.
Stage Four: Cross-Purpose Medicine and the Formalization of Public Data
Formal drug repurposing — what researchers since a landmark 2004 paper by Ted T. Ashburn and Karl B. Thor have called “drug repositioning”[13] — enters as the final stage of this sequence.
By the time a manufacturer funds formal repurposing trials for a secondary indication, the safety and efficacy profile has typically been “roughed out” by years of off-label use at public expense and public risk. At this point, the requisite, token, formal clinical trial is, in significant part, a pro forma regulatory codification of data that was generated without structured consent architecture and without compensation to the patients who generated it.
This does not necessarily mean that repurposing trials are entirely without value. In theory, they impose rigorous protocols, placebo controls, and statistical standards for which real-world observational data cannot entirely be a substitute.
But, it is nonetheless worth noting that a manufacturer’s investment has been substantially de-risked at this stage by the preceding population-level experience and surveillance — all of which were, once again, generated at little to no discernible cost to the manufacturer, and at non-negligible physical risk to patients who were not formally enrolled in a research program.
Building the Machine
The preceding stages describe a recurring pattern of risk transfer as it operates in practice. But institutional processes do not emerge spontaneously. They are enabled by legal doctrines, legislative interventions, judicial decisions, and ideological assumptions that make particular incentive structures possible while foreclosing others.
If the preceding sections examined the machine in motion, the next sections examine how it was assembled. The liability-laundering system was not created all at once, nor by any single actor. Rather, it emerged incrementally through decades of changes to patent law, pharmaceutical regulation, commercial-speech doctrine, and prevailing assumptions about the proper relationship between public institutions and private enterprise.
To understand why risk flows through the system as it does, one must first understand the architecture that channels it.
The Legal Architecture
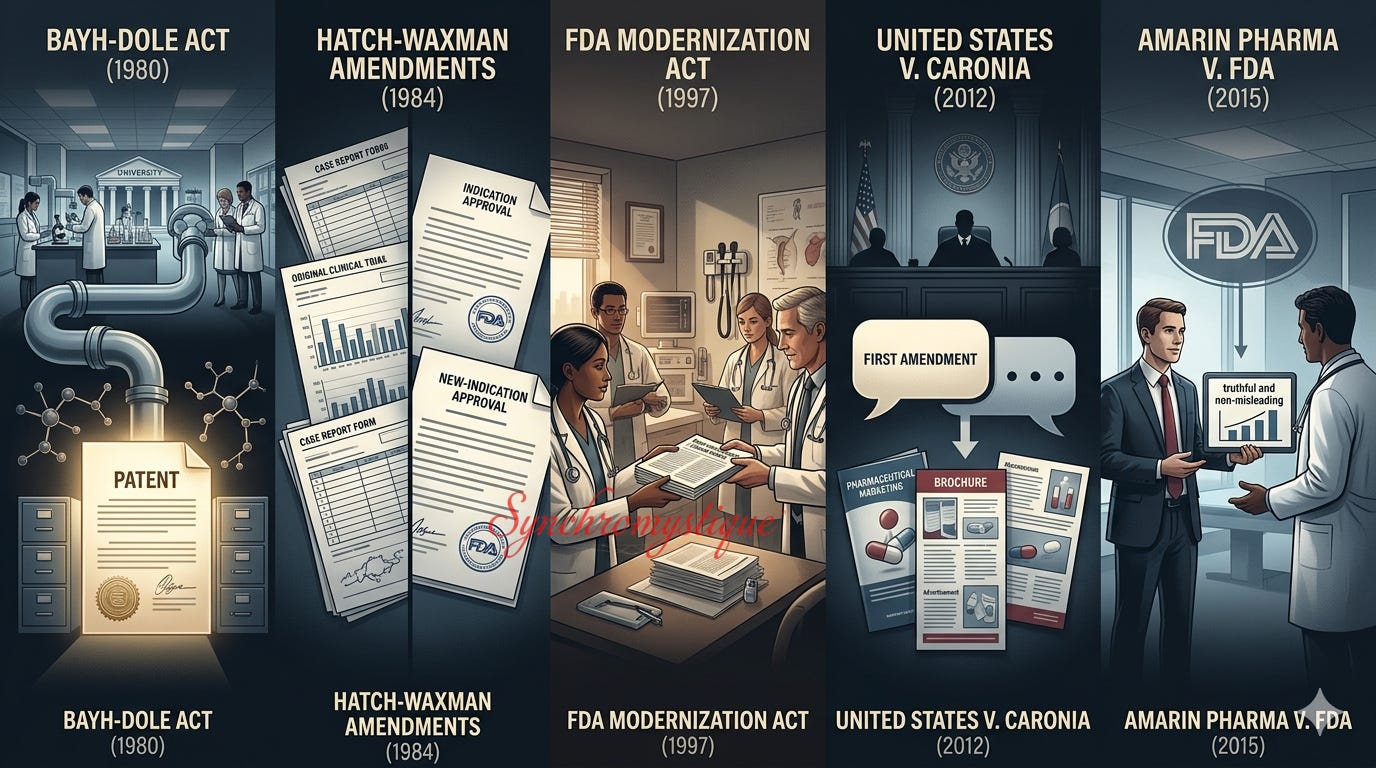
The liability shield described above was not always as robust as it is today. It was constructed through targeted legal and legislative intervention across four decades.
The previously mentioned Bayh-Dole Act (1980) established the pipeline from public research to private patent.
The Hatch-Waxman Amendments (1984) created the 505(b)(2) regulatory pathway that allows new-indication approvals without full repetition of the original safety trials.
The FDA Modernization Act (1997) temporarily permitted manufacturers to distribute peer-reviewed journal articles on unapproved uses to physicians — and, thus, was a statutorily underwritten mechanism for encouraging off-label prescribing.
United States v. Caronia[14] (2012) extended First-Amendment commercial-speech protection to “truthful” off-label promotion, substantially limiting the FDA’s practical enforcement capacity.
Amarin Pharma v. FDA[15] (2015) extended the previous reasoning further, preventing the FDA from prosecuting manufacturers for proactive off-label marketing — again, as long as statements were “truthful.”
We feel that we owe the reader an account of why that seemingly straightforward word — truth — is in scare quotes. As it happens, both Caronia and Amarin condition First-Amendment protection on promotional statements being “truthful.” But the standard of truthfulness the courts apply is, in effect, a sincerity-and-non-fabrication test. The claim in view must be traceable to real data and must not be literally false. What it need not be is accurate in the more demanding sense that the FDA’s own approval process requires — namely, supported by the weight of evidence from adequate, well-controlled, independently replicated clinical trials.
The result is a constitutionally protected gap between the evidentiary threshold for approving a new indication and the evidentiary threshold for promoting one even without approval.
A manufacturer may not market a use that it has not — and perhaps could not — get approved. Nevertheless, it may promote that same use provided it can point to some supporting data or other — however selectively assembled.
Technically non-false and genuinely well-supported are not the same standards. The First Amendment, as applied to and interpreted in these decisions, merely protects the public from the former. Meanwhile, the public itself, reasonably, generally assumes that the courts are guaranteeing or safeguarding the latter.
The cumulative effect is a legal architecture in which the practical barriers to off-label market expansion have been systematically reduced or removed, while the liability shields available to manufacturers have been systematically multiplied and strengthened — not through any single coordinated act, but through the ongoing operation of (instrumentally) rational institutional actors within an incentive structure that rewards exactly these outcomes.
Friedman’s ‘Rules of the Game’
Milton Friedman (in-)famously argued in 1970 that the social responsibility of business is simply to increase profits — provided only that firms operate within the “rules of the game.”
In Friedman’s (originally Neoliberal, later right-libertarian) lexicon, these “rules” were basically reduced to those necessary (in his view) to referee open competition without deception or fraud.
It is worth pausing on that qualifier. The structural argument traced above suggests that the pharmaceutical industry has not merely played within static, preëxisting rules, but that it has substantially rewritten those rules to more “efficiently” increase its profits.
For example, it lobbied for the legislative interventions that created the Bayh-Dole pipeline; it litigated the judicial expansions that converted the First Amendment into a commercial-speech shield; and it shaped the regulatory apparatus that transformed the package insert from a mere disclosure requirement into an arguably covert liability-transference instrument.
If the rules themselves are the product of the regulated industry’s political influence, then even Friedman’s framework — applied without selective quotation — does not vindicate the outcome. It arguably condemns it.
There is a further irony.
Friedman objected to corporate “social responsibility” rhetoric on the grounds that it amounted to executives spending shareholders’ money on unauthorized public goals. But the Nader Loop describes something structurally symmetrical yet opposite: namely, an industry spending the public’s money — channeled through NIH grants and university research budgets — to generate discoveries that are then privatized through exclusive licensing. In Friedman’s own terms, this is an involuntary transfer of public resources to private shareholders, conducted entirely without democratic authorization. Thus, the Chicago School’s most famous soundbite, read carefully, seems to provide ammunition for the critique it is most often recruited to deflect.
Conclusion: Our Synthetic Claim
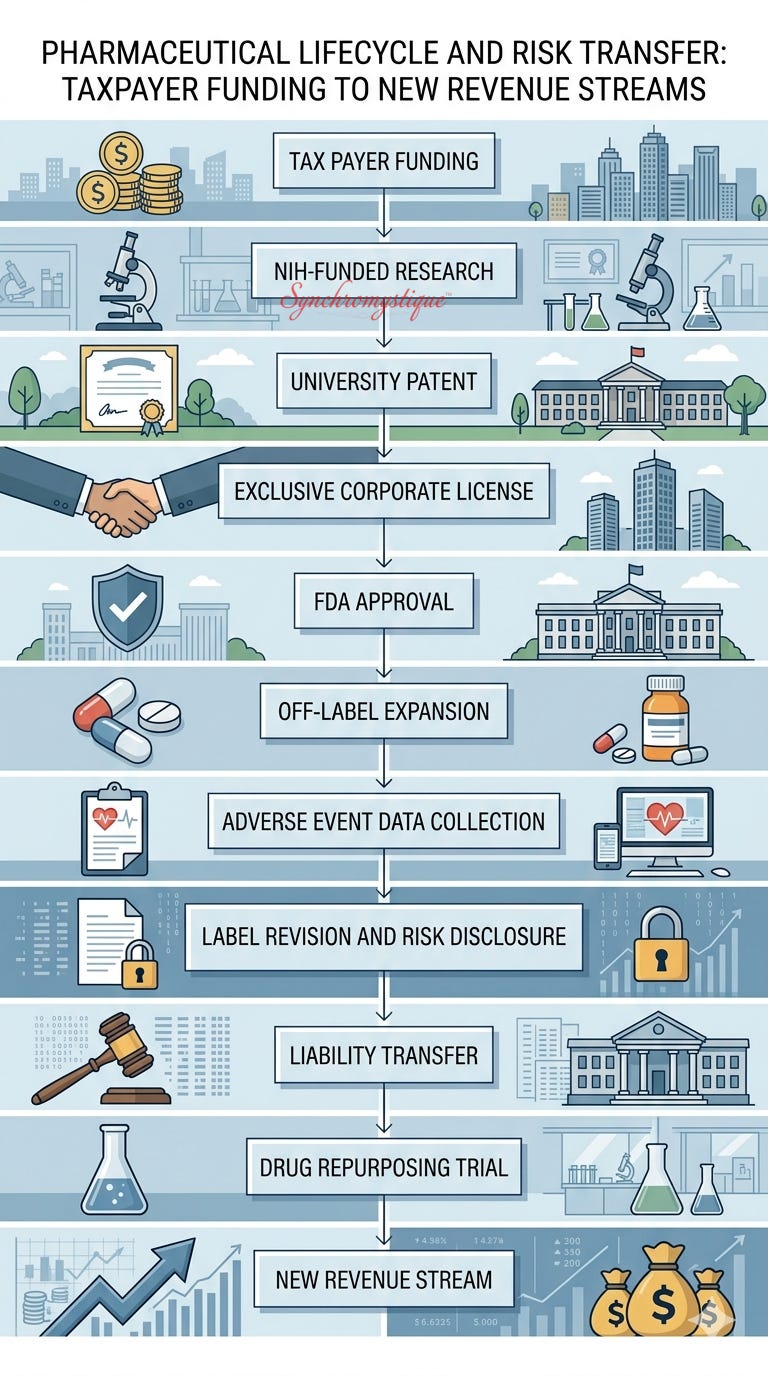
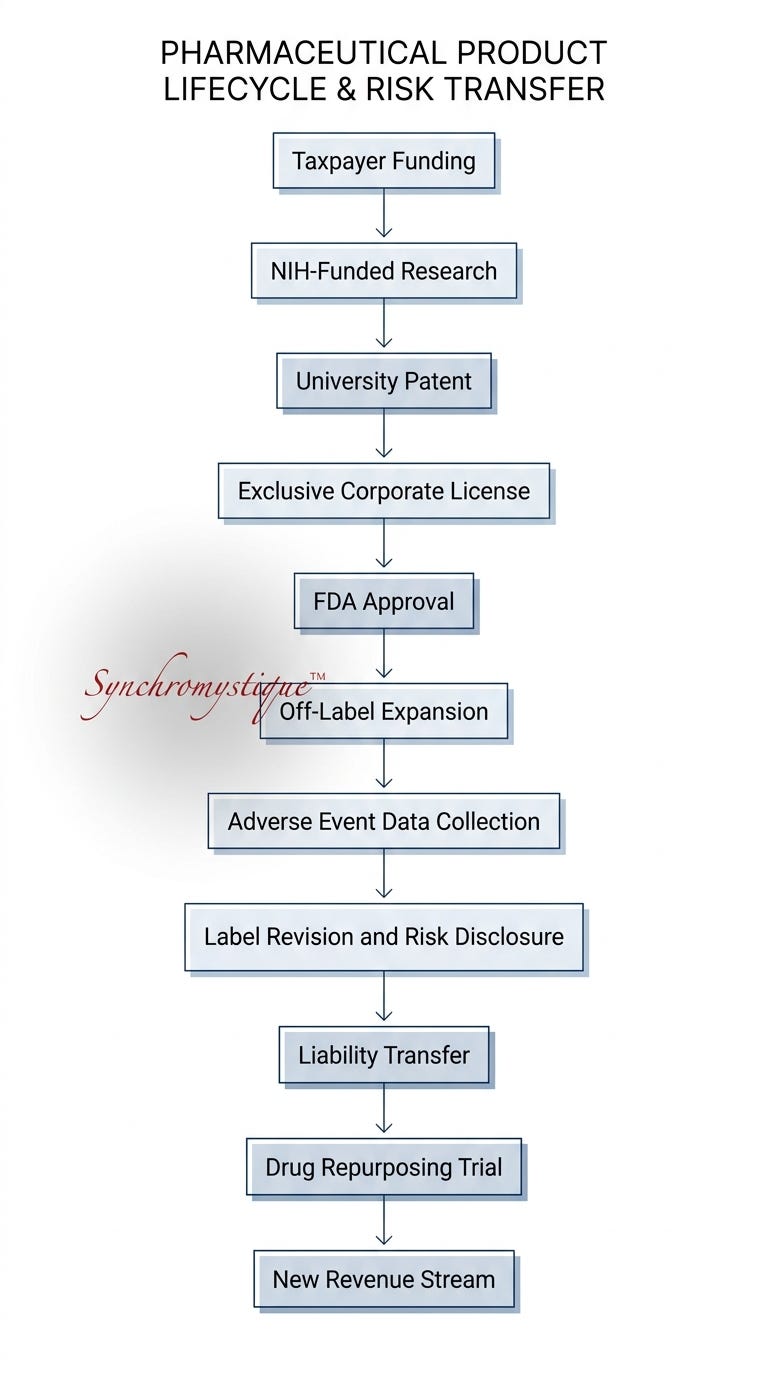
Our argument is that the five stages sketched above are not parallel problems. They are sequential components of a single institutional process.
Publicly funded research identifies some commercially promising chemical molecules.
The science is then “licensed” to private pharmaceutical companies which then file New-Drug Applications to obtain initial approvals for some primary indications.
Off-label prescribing then paves the way for indications expansion by stress-testing those drugs on large populations outside formal research safeguards and with liability falling largely on physicians.
Adverse data collected via off-label surveillance is then incorporated into the drug’s “label” (i.e., the package insert), completing a liability transfer to physicians and, ultimately, to patients themselves.
Only then are formal repurposing trials engineered — effectively monetizing what the public already paid for twice: once to discover and again, in physical risk, to test.
At each stage, the institutional architecture systematically reduces, redistributes, or externalizes significant categories of risk that might otherwise remain concentrated on manufacturers. From the point of view of (instrumental) rationality, the industry has no obvious incentive not to exploit these institutional structures to the utmost.
The patient, in the most precise available terms, is simultaneously the system’s funder, its test population, its legal shock absorber, and — at the end of the day — its customer.
Appendix: How Did It Come to This?
The preceding analysis deliberately remained at the level of institutions, incentives, legal doctrines, and observable historical developments.
We have argued that the modern pharmaceutical system exhibits a recurring tendency to transfer costs, liabilities, and risks away from manufacturers and toward the public.
But describing a pattern is not the same thing as explaining it.
Why should such patterns emerge at all? Why do institutions that are ostensibly designed to protect the public so often (d)evolve into mechanisms that appear to serve the interests of the organizations that they supposedly “regulate”? And why does this process recur across sectors, political administrations, and generations of policymakers?
The appendix that follows steps back from the pharmaceutical industry itself and turns toward several intellectual traditions that have attempted to answer questions of this kind.
Although their conclusions often differ dramatically, Frankfurt School so-called “critical theorists,” “public-choice” economists, and critics of neoliberalism all grappled with a common problem: namely, how it could be that complex institutions acquire a momentum and internal logic that seem to transcend the intentions of the individuals who inhabit them.
Three Explanations of Institutional Behavior
The traditions surveyed below differ sharply in their political commitments and conclusions. Yet all of them, in one way or another, grapple with (versions of) the same underlying question: How do institutions come to exhibit persistent patterns of behavior that cannot be adequately explained by the motives of any particular individuals within them?
The concepts introduced in this section are offered not as additional evidence for the preceding analysis, but as possible explanatory frameworks through which its recurring themes may be interpreted.
The Frankfurt-School Diagnosis
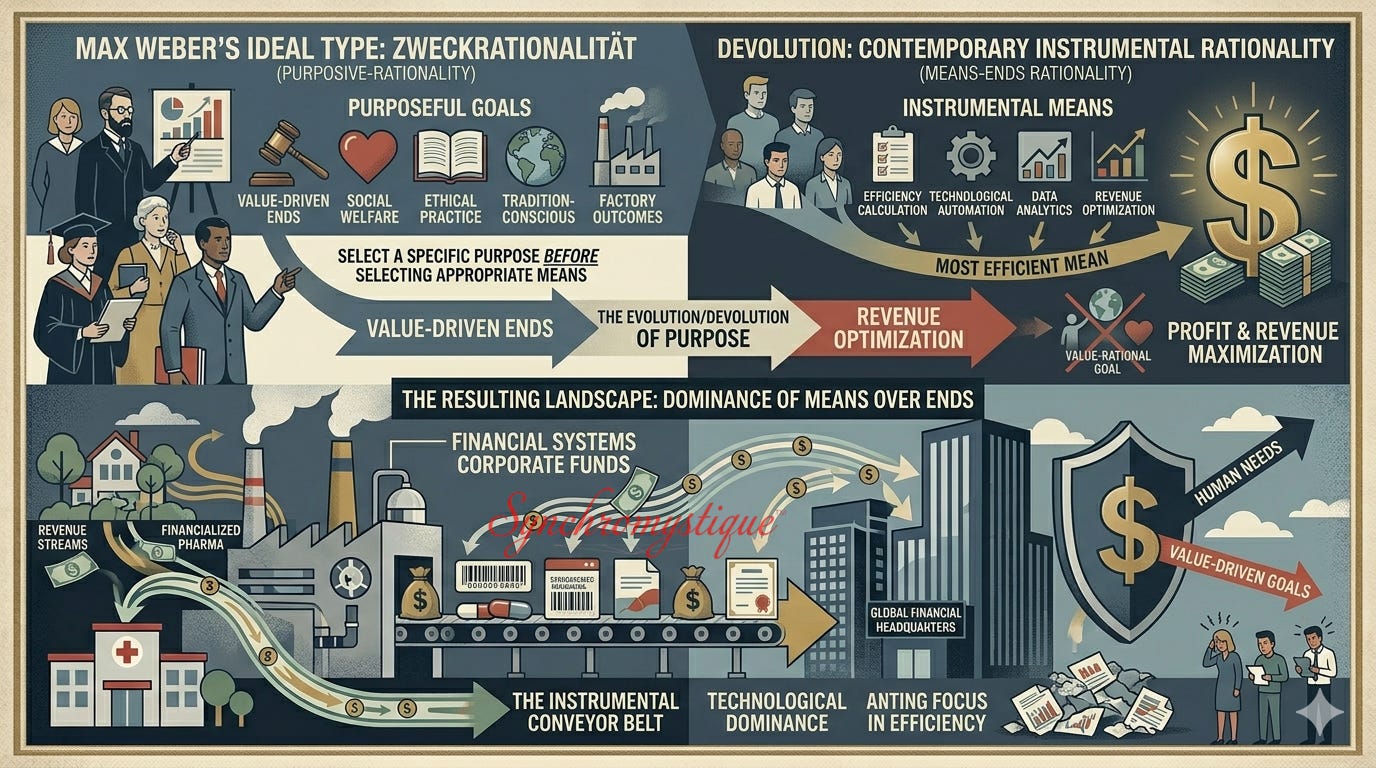
The “rationality” that the essay consistently criticizes is not to be caricatured as irrationality, stupidity, or malice. It is, in the precise vocabulary of critical theory, instrumental rationality — or what German sociologist Max Weber called Zweckrationalität, the rationality of means-ends calculations that are detached from any moral evaluation of ends themselves. Weber identified this as the defining characteristic of modern bureaucratic and capitalist institutions. It is a form of reasoning that is extraordinarily efficient at achieving its predefined objectives. But it is structurally indifferent to whether those objectives are just, humane, or socially beneficial.
Herbert Marcuse, Max Horkheimer, and Theodor Adorno, writing in the tradition Weber opened, argued — the latter in Dialectic of Enlightenment (1944) and the former in One-Dimensional Man (1964) — that instrumental rationality had become the dominant mode of thought in modern industrial societies. They worried that this had become not merely an economic phenomenon but a civilizational one, and that the capacity for substantive moral reasoning had been progressively “colonized” by means-ends calculations.
Jürgen Habermas later refined this diagnosis. In his 1981 The Theory of Communicative Action, he described the “colonization of the lifeworld” by systems logic as a process by which domains of human activity that ought to be governed by ethical deliberation (medicine, law, democratic governance) are instead progressively reduced to administrative or market considerations.
The pharmaceutical system is a case study in precisely this “colonization.”
The package insert that should function as a public-health disclosure functions instead as a corporate-liability shield.
The clinical trial that should function as a truth-seeking procedure functions instead as a risk-transfer mechanism.
The regulatory agency that should function as a public watchdog functions instead (through capture) as rule-legitimation, subservient to the industry it nominally “oversees.”
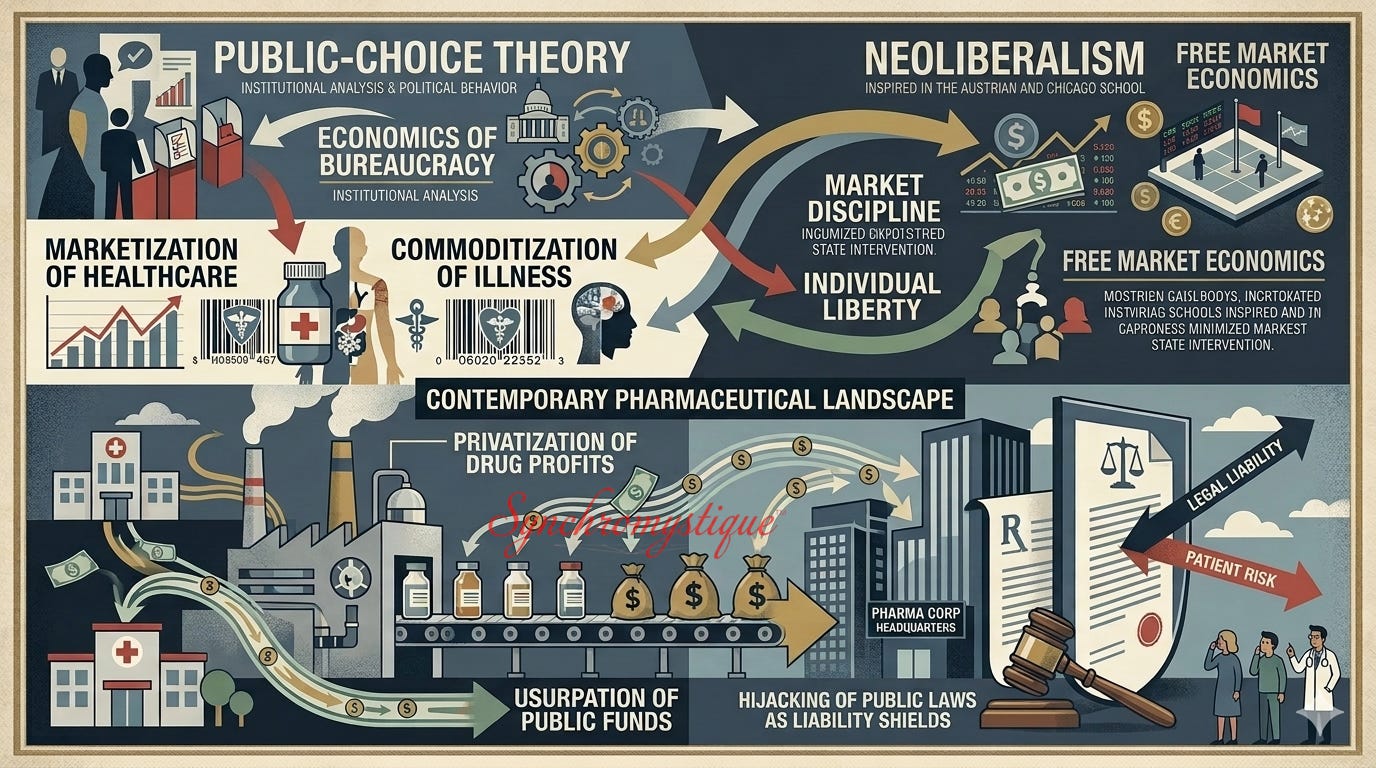
The Public-Choice Complication
Public-Choice Theory, developed by such 20th-century American economists as James McGill Buchanan, Jr.[16] and Gordon Tullock from the 1960s onward,[17] arrived at a structurally similar description of institutional behavior through an alternate ideological route. Where the Frankfurt critics saw institutional instrumental rationality as a pathology to be diagnosed and treated, Buchanan and Tullock presented it as a neutral empirical fact about human nature — including government actors — to be accommodated or constrained through constitutional design.[18]
The public-choice insight most relevant for our purposes is the idea of regulatory capture. The observation is that regulatory agencies, staffed as they are by self-interested actors who operate in proximity to the industries that they are tasked to regulate, tend — over time — to serve those industries’ interests rather than the public’s.

This is not a “conspiracy theory.” A glance at the historical record shows how routinely this revolving-door phenomenon — where individuals alternate between highly lucrative private sector positions and the public agencies tasked with oversight — plays out across sectors.
In finance, critics point to figures such as Scott K. H. Bessent (under Trump); Walter Joseph “Jay” Clayton III (also under Trump); Timothy Franz Geithner (under Obama); Gary Scott Gensler (Biden); Jacob Joseph “Jack” Lew (Obama); Howard William Lutnick (Trump); Henry Merritt “Hank” Paulson (George W. Bush); Dina Powell (George W. Bush and Trump); Robert Edward Rubin (Clinton); and Steven Terner Mnuchin (Trump), whose careers trace a now all too familiar arc between Wall Street (often especially, but not exclusively powerhouse firm Goldman Sachs) and the federal agencies charged with overseeing it. This dynamic can — and does — tilt policy toward the stability and profitability of incumbent firms rather than the public interest.
Yet the same pattern appears with arguably even greater clarity in the pharmaceutical and public‑health sphere, where the stakes include not only “market outcomes” but the nation’s biomedical infrastructure — to say nothing of our wellbeing as individuals.[19]
Former Centers for Disease Control and Prevention (“CDC”) Director Julie Gerberding moved directly to head Merck’s vaccine division;
Former FDA Commissioner Scott Gottlieb joined Pfizer’s board merely three months after resigning;
Former FDA head Stephen Hahn entered the venture‑capital firm behind Moderna; and
Senior public‑health leaders such as Mandy Cohen, Francis Collins, and Anthony Fauci have been scrutinized for institutional arrangements in which federal agencies both “regulate” and profit from pharmaceutical innovation.
The symmetry across sectors (which we have only gestured toward) underscores the public‑choice point. But the pharmaceutical examples sharpen it, because they reveal how regulatory capture can operate not only through personnel flows but also through structural incentives embedded in the machinery that produces publicly funded biomedical research.
Taken together, these cases (and numerous others besides) illustrate that what public‑choice theory predicts is not episodic “misconduct,” but a durable structural tendency. It’s a feature of the System — not a “bug.”
This trajectory becomes especially visible, and tremendously consequential, in domains like pharmaceutical manufacturing where regulatory decisions and commercial incentives are tightly interwoven. It is, moreover, a prediction that follows straightforwardly when the assumption of self-interested instrumental rationality is applied as consistently to bureaucrats and regulators as to corporate executives.
The irony is that public-choice theory was deployed historically as an argument against regulatory intervention. If regulators can be captured, the argument ran, then regulation produces worse outcomes than markets. But the case of pharmaceuticals demonstrates a far less comfortable implication that public-choice theorists have been slower to acknowledge: The same reasoning that predicts regulatory capture also predicts academic capture, legislative capture, and judicial capture.[20]
If all human actors whatsoever are — literally by nature[21] — both instrumentally rational as well as self-interested, then the rules of the game are themselves the products of instrumental rationality applied in the pursuit of somebody’s self-interest.
The question seldom asked is: Cui bono?
Buchanan’s own framework (applied without selective quotation), does not vindicate the outcomes described in this essay. But it does suggest an explanation for them — which is a different (and arguably even more damning) contribution.
The Neoliberal Connexion
Neoliberalism — as an ideological and policy program associated with “Austrian Economist” Friedrich Hayek, “Chicago School” thinker Milton Friedman, and their institutional infrastructure of think tanks, foundations, and law schools[22] — provided the political vehicle through which public-choice rationality was converted from academic theory into actual governmental practice.
The specific legislative interventions traced in this essay’s timeline (Bayh-Dole, Hatch-Waxman, FDAMA, the Caronia and Amarin decisions) did not emerge from a neutral technocratic process. They emerged from a concerted, ideologically coherent, sustained, and well-funded, campaign to restructure the relationship between the state, the market, and the individual. The aim was to anti-progressively redefine the state’s rôle from being the guarantor of public welfare to a mere enforcer of “private” (read: corporate) contract and intellectual property rights.[23]
Friedman’s previously cited 1970 aphorism — that “the social responsibility of business is to increase profits,” within the rules of the game — is the ideological catalyst of this transformation.
As we have argued, Friedman’s dictum, despite its crucial qualifier (“within the rules”) does no limiting work when the industry in question wrote (or at least helped write) the rules.
Given this, the Chicago School’s most cited soundbite, read carefully, provides a basis on which to condemn the pharmaceutical system’s behavior rather than vindicating it — because the rules of the game, in this sector, are not the output of “open” or “free” competition. They are the output of sustained, well-financed lobbying by the very actors the rules are supposed to constrain. That the actors are to be credited as being (instrumentally) “rational” seems to us to be an indictment of any analysis of means that abstracts from, ignores, or objects to the evaluation of ends.
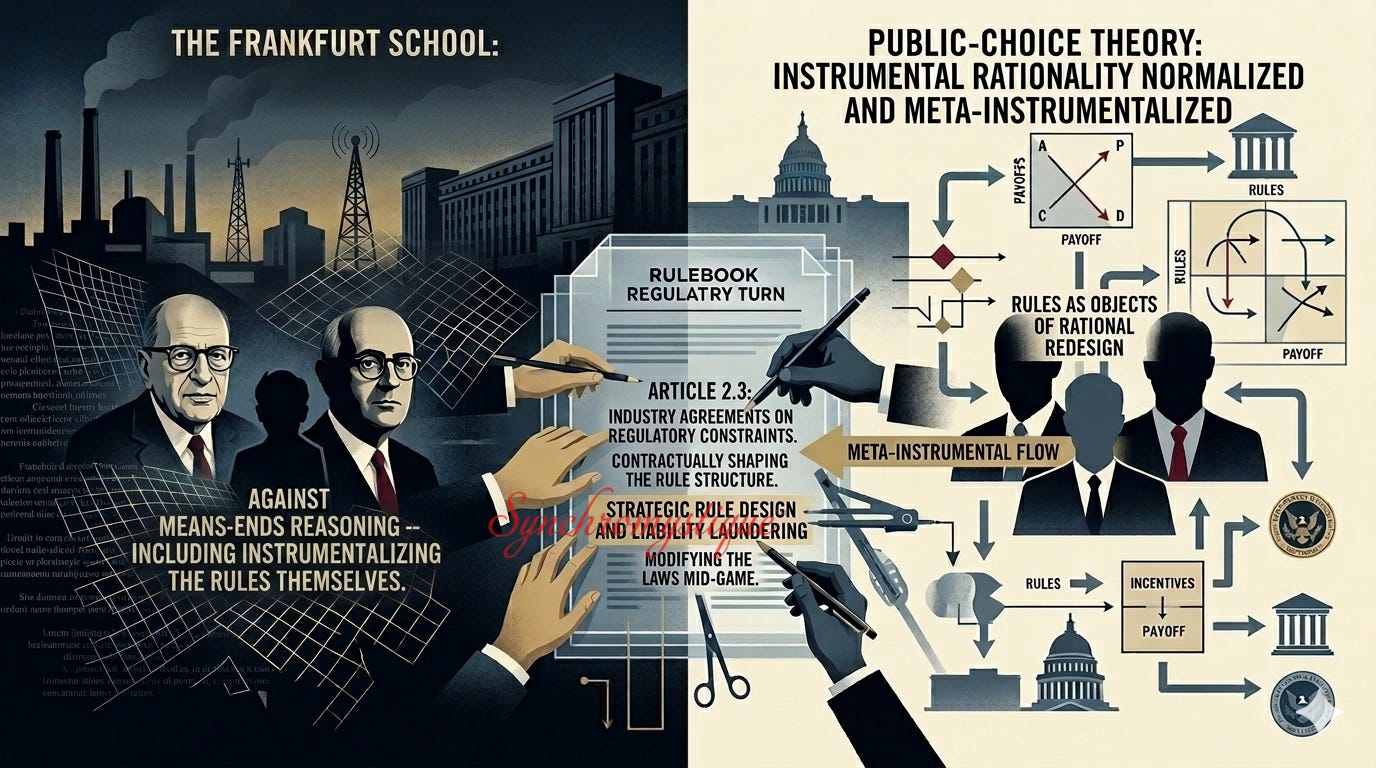
The Meta-Instrumental Turn
There is one further development worth naming. Standard instrumental rationality describes agents pursuing goals efficiently within a given rule structure. What our Friedman section identifies is something rather more insidious (if also sophisticated): There is no more “given.”
This process is what you might call meta-instrumental rationality, in which agents rationally invest in modifying the rule structure itself.
The pharmaceutical industry’s lobbying for Bayh-Dole, its litigation strategy in Caronia and Amarin, its shaping of FDA accelerated approval pathways — these are not merely instances of “playing within the rules.” They are investments in rewriting the rules to make subsequent play more profitable.
This is, arguably, the most structurally salient feature of the liability-laundering system, and the one least susceptible to reform through ordinary regulatory tightening. This is because any new regulatory constraint itself becomes an immediate target for the same meta-instrumental rationality that shaped the existing constraints.
The upshot is that the patient who enters this system does so as a consumer in a market that was designed by its most powerful participant. That this design required no conspiracy — only the consistent, (instrumentally) “rational” pursuit of institutional self-interest by actors operating across decades and across the legislative, judicial, and regulatory branches simultaneously — is not a mitigating or peripheral observation. It is, we think, the most incriminating one available.
Affiliate Disclosure
Some of the URLs above (or in the end notes, below) may be Amazon-affiliate links. As an Amazon Associate, I earn from qualifying purchases — at no additional cost to you.
Please note that, if you choose to purchase through these links, you’re not just acquiring a single book or resource; you’re also helping support The SynchroMystic (Substack.com/@MatthewJBell) and making possible further explorations into crypto-politics, crypto-economics, Jungian synchronicities, occult oddities, and the broader philosophical-theological currents that weave through our publications.
Your support helps keep the signal flowing. Thank you.
End Notes:
[1] The rationality in view throughout this analysis is what 19th-20th-century German sociologist Max Weber termed Zweckrationalität — instrumental rationality — and what Frankfurt School theorists such as Theodor Adorno, Max Horkheimer, and Herbert Marcuse later identified as the defining pathology of modern institutional life: the systematic subordination of moral and social ends to the efficient pursuit of predefined goals, typically profit or organizational self-preservation. Crucially, we are not discussing individual psychology but institutionalized “rationality” — defined as behavior that the incentive architecture of a legal and regulatory system makes not merely possible but, for any actor operating within it, effectively mandatory. Once again, we emphasize: our critique is structural, not conspiratorial: the system does not require “villains.” It requires only agents behaving instrumentally rationally within rules that were themselves shaped by prior (or contemporary) rational agents pursuing the same ends.
[2] This is according to the assessment of its critics, from Ralph Nader to institutional economists studying regulatory capture (a critical trajectory popularized on the short-lived 2024 campaign trail by Robert Francis Kennedy, Jr.)
[3] Ekaterina Galkina Cleary, Jennifer M. Beierlein, Navleen Surjit Khanuja, and Fred D. Ledley, “Contribution of NIH funding to new drug approvals 2010–2016,” Solomon H. Snyder, ed., PNAS, vol. 115, no. 10, Baltimore, Md.: Johns Hopkins Univ. School of Medicine, Feb. 12, 2018, pp. 2,329-2,334, <https://doi.org/10.1073/pnas.1715368115> and <https://www.pnas.org/doi/abs/10.1073/pnas.1715368115>.
[4] A “compound library” is a real catalog of chemicals designed for high‑speed testing (this is the “screening” part) to find molecules that affect a disease target.
[5] The act — named after co-sponsoring Senators Birch Bayh and Bob Dole — let universities, nonprofits, and small businesses keep patent rights to inventions that had been developed with federal funding. It created a pipeline for technology transfer which was rationalized as unlocking the economic value of “dormant” research on the theory that inventors themselves — not the federal government — were best equipped to turn taxpayer‑funded discoveries into real-world products. As to why this effective divestment didn’t result in a wave of public indignation, this was partially because it was framed as a technical “efficiency” reform and because the government retained “march‑in rights” which (it claimed) ensured that publicly funded inventions would “serve the public interest.” Although it wasn’t “deregulation” in the strict Reaganite sense (it was was signed into law by President Jimmy Carter on Dec. 12, 1980), it was a key early step in the broader late‑20th‑c. shift toward “marketizing” public research — an ideological shift that harmonized with, and helped set the stage for, Reagan‑era deregulation. In retrospect, it marked a move toward neoliberal and public‑choice frameworks — privatizing the outputs of public research and embedding “market logic” inside a university system already drifting toward a “human‑capital” orientation. Human‑capital Theory recast education as an individual economic investment that (supposedly) enhanced a graduate’s productivity and future earning power. If the student was the primary beneficiary, this logic held, then the student should also bear the costs and risks — a shift mirrored in the broader transfer of risk from employers to employees through the replacement of defined‑benefit pensions with 401(k)s. This investment‑oriented view did not displace a fully Deweyite university ethos — not least because higher education had never truly operated on Dewey’s democratic, civic, or experiential model. Instead, it supplanted an older, largely implicit “sorting” regime in which universities functioned as filters for employers — signaling intelligence, discipline, or class background more than cultivating democratic character. Dewey’s vision did however reshape K-12 schooling far more than it did universities, which long combined elite civic formation with the German research model (which prioritized specialized, objective, and detached scientific research over student-centered holistic growth; think Johns Hopkins). Human‑capital theory therefore did not overthrow a Deweyite university system so much as it formalized and intensified a preëxisting shift: Moving from education as a public good and as civic preparation and toward education as a private investment and as an enhancement to one’s labor‑market credentials or a flourish to one’s résumé. Nevertheless, since it dovetails with our main themes, we may as well state that whereas Dewey saw education as intrinsically valuable (a foundation of democracy), human‑capital theory reframed it as instrumentally valuable (a supposed pathway to private wealth).
[6] Nader founded the Washington, D.C.-based Public Citizen as a progressive, non-profit, consumer-rights advocacy group and think tank in 1971.
[7] Ralph Nader, Cutting Corporate Welfare, New York: Seven Stories Press, 2000, p. 59, <https://books.google.com.na/books?id=fjfT4M-_cW4C>.
[8] <
https://www.citizen.org/?s=bayh-dole
>.
[9] See press release, U.S. Department of Justice, May 13, 2004, <https://www.justice.gov/archive/opa/pr/2004/May/04_civ_322.htm> and Christian J. Krautkramer, “Neurontin and Off-Label Marketing,” AMA Journal of Ethics (American Medical Association), Jun. 2006, <https://journalofethics.ama-assn.org/article/neurontin-and-label-marketing/2006-06>.
[10] See press release, U.S. Department of Justice, Jan. 15, 2009, <https://www.justice.gov/archive/opa/pr/2009/January/09-civ-038.html> and “Eli Lilly pays record $1.4bn for promoting off-label use of olanzapine,” TheBMJ (British Medical Journal), vol. 338, Jan. 20, 2009, <https://doi.org/10.1136/bmj.b217> and <https://www.bmj.com/content/338/bmj.b217>.
[11] See civil complaint, U.S. Attorney’s Office, Oct. 26, 2011, <https://www.justice.gov/sites/default/files/opa/legacy/2012/07/02/us-complaint.pdf> and “GlaxoSmithKline to Plead Guilty and Pay $3 Billion to Resolve Fraud Allegations and Failure to Report Safety Data,” press release, U.S. Department of Justice, Jul. 2, 2012, <https://www.justice.gov/archives/opa/pr/glaxosmithkline-plead-guilty-and-pay-3-billion-resolve-fraud-allegations-and-failure-report>.
[12] Russell G. Thornton, “The Learned Intermediary Doctrine and Its Effects on Prescribing Physicians,” Proc Bayl Univ Med Cent (Baylor Univ. Medical Ctr. Proceedings), vol. 16, no. 3, Jul. 2003, pp. 359-361, <https://pmc.ncbi.nlm.nih.gov/articles/PMC1200796/>. Cf. Sterling Drug v. Cornish (370 F.2d 82, 85), 1966.
[13] Ted T. Ashburn and Karl B. Thor, “Drug Repositioning: Identifying and Developing New Uses for Existing Drugs,” Nature Reviews Drug Discovery, vol. 3, no. 8, Aug. 2004, pp. 673-83, <https://pubmed.ncbi.nlm.nih.gov/15286734/>. Cf. Joris Langedijk, Aukje K. Mantel-Teeuwisse, Diederick S. Slijkerman, and Marie-Hélène D.B. Schutjens, “Drug Repositioning and Repurposing: Terminology and Definitions in Literature,” Drug Discovery Today, vol. 20, no. 8, Aug. 2015, pp. 1,027-1,034, <https://www.sciencedirect.com/science/article/abs/pii/S1359644615001774>.
[14] United States v. Caronia, 703 F.3d 149 (2d Cir. 2012).
[15] Amarin Pharma, Inc. v. United States Food & Drug Administration, 119 F. Supp. 3d 196 (S.D.N.Y. 2015).
[16] Not to be confused with 19th-century statesman James Buchanan, Jr. who was the 15th U.S. president.
[17] Public Choice Theory holds that political actors respond to incentives: Buchanan emphasized the constitutional rules that structure those incentives; Tullock alleged that actors systematically exploit the rules through “rent‑seeking”; and political scientist Mancur Lloyd Olson, Jr. thought he could explain why small, organized groups succeed in rewriting rules, while the general public fails to defend its interests.
[18] Something of an earlier thought along the same lines might be ascribed to the Founding Father, and third U.S. president, Thomas Jefferson, who wrote: “In questions of power, then, let no more be heard of confidence in man, but bind him down from mischief by the chains of the Constitution.” . Thomas Jefferon, “Jefferson’s Draft [of the Kentucky Resolutions,” before Oct. 4, 1798, Founders Online, National Archives, <https://founders.archives.gov/documents/Jefferson/01-30-02-0370-0002>; citing Barbara B. Oberg, ed., The Papers of Thomas Jefferson, vol. 30, Jan. 1, 1798 - Jan. 31, 1799, Princeton, N.J.: Princeton Univ. Press, 2003, pp. 536-543.
[19] Of course, financial outcomes are themselves responsible for creating conditions of despair and misery that correlate with (minimally) or produce (maximally) negative health outcomes — including untold death.
[20] According to Noam Chomsky: “… there are stenographers to power. [American diplomat and theorist Henry Alfred] Kissinger, a master in the art, put it pretty well himself. He said the role of the policy intellectual is to articulate the thinking of those in power, ‘elaborating and defining’ their ‘consensus.’ If they [i.e., the powerful] don’t put it exactly right, we’ll [i.e., the intellectuals will] articulate it correctly for them. That’s the role of the serious intellectual. And that’s how you become a respected, responsible intellectual.” Noam Chomsky, “Marx’s Old Mole is Right Beneath the Surface,” David Barsamian, interviewer, Alternative Radio; Boston Review, Apr. 8, 2021, <https://chomsky.info/20210408-2/> and <https://bostonreview.net/class-inequality-politics/noam-chomsky-david-barsamian-mole>. As far as I have been able to determine, Kissinger never publicly wrote or said precisely the sentence that Chomsky seems to attribute to him. It is important to note, however, that the remarks reproduced above are almost certainly transcriptions of a spoken interview. Therefore, the embedded quotation marks are interpretive interpolations — unless Chomsky mimed “air quotes” as he spoke. All that said, even though the exact wording is almost certainly Chomsky’s paraphrase, the sentiment is authentically Kissingerian. For example, during the late 1950s and early 1960s, Kissinger described “experts” as defining the range of “acceptable” policy, elaborating and making explicit underlying strategic assumptions, and — as Chomsky says — providing conceptual coherence to whatever the “ruling consensus” happens to be.
[21] We wish to register our objection to metaphysical nominalists (or anti-realists) helping themselves to a “human nature.” But, we lack the time to develop the point.
[22] We are referring to the postwar, Neoliberal-institutional network centered on the Mont Pelerin Society and its affiliates (e.g., the Institute of Economic Affairs, Manhattan Institute, and Atlas Network), all of which were supported by a transatlantic bloc of business‑funded foundations (e.g., the Bradley, Earhart, John M. Olin, Koch family, and Scaife Foundations, the Volker Fund, etc.), and anchored academically in the University of Chicago and related law‑and‑economics programs.
[23] This is the point at which the entire corporate-law apparatus — including many “lobbying” firms — attaches itself.